Cavalier King Charles Spaniels
Est. 1976
Hips & Patellas
|
HIP DYSPLASIA is a common cause of
rear-end lameness in the dog. The problem lies in the structure
of the joint. The head of the femur (thigh bone) should sit
solidly and tightly in the acetabulum (cup). In hip dysplasia
loose ligaments allow the head to begin to work free. A shallow
acetabulum also predisposes to joint laxity. Finally, the mass
or tone of the muscles around the joint socket is an important
factor.
Tight ligaments, a broad pelvis with a well-cupped acetabulum,
and a good ratio of muscle mass to size of bone, predispose to
good hips. The reverse is true of dogs who are likely to develop
the disease. Environmental factors, including weight and
nutrition of the puppy and rearing practices figure into the
final outcome. Keeping a growing puppy lean and on a good diet
will greatly mask and may even prevent the symptoms of hip
dysplasia.
Above are examples of hip x-rays of two different Cavaliers. If
you compare the two you can see that the hip sockets on the
right x-ray are not as deep as those on the left x-ray,
therefore the femoral heads do not sit as deeply into the
sockets—more of the femoral head is left out of the socket.
Also, in the dysplastic x-ray, you can see the circled hip is
much worse than the other hip. The end of the femoral head is
already worn down. Because of stress, the area pointed to behind
the femoral head has filled in so much the indentation is nearly
gone. Compare this to the other three hips that have good
indentation behind the femoral head. NOTE: the dog with the
dysplastic hips showed NO signs of hip dysplasia when walking
or running. The x-ray was taken only because the owner wanted to
make sure the dog did not have hip dysplasia before it was bred.
Since the dog does have hip dysplasia, the breeder decided not
to breed the dog. Also, BOTH parents are OFA clear of hip
dysplasia, and so is the one other sibling whose hips have been
x-rayed and sent to OFA.
Hip dysplasia is a moderately heritable condition. It is more
likely among littermates having a dysplastic parent, but even
dogs with normal hips can product dysplastic pups.
However—consistently breeding unaffected dogs WILL reduce the
incidence of hip dysplasia, especially if the hip status of
littermates is taken into consideration.
According to OFA statistics, approximately 10-11% of all
Cavaliers develop hip dysplasia by 2 years of age. Please note
that this figure is considerably lower than the true incidence
as the vast majority of breeders do NOT send in x-rays that show
obviously dysplastic hips. The widely accepted guess is that the
incidence is probably about twice as high as what the OFA
statistics show. Again, this is a developmental defect. Puppies
are NOT born with hip dysplasia. Some dogs with x-ray evidence
of even severe hip dysplasia show NO clinical signs (no pain or
lameness), so the disease may remain entirely unsuspected unless
an x-ray is taken to check for it.
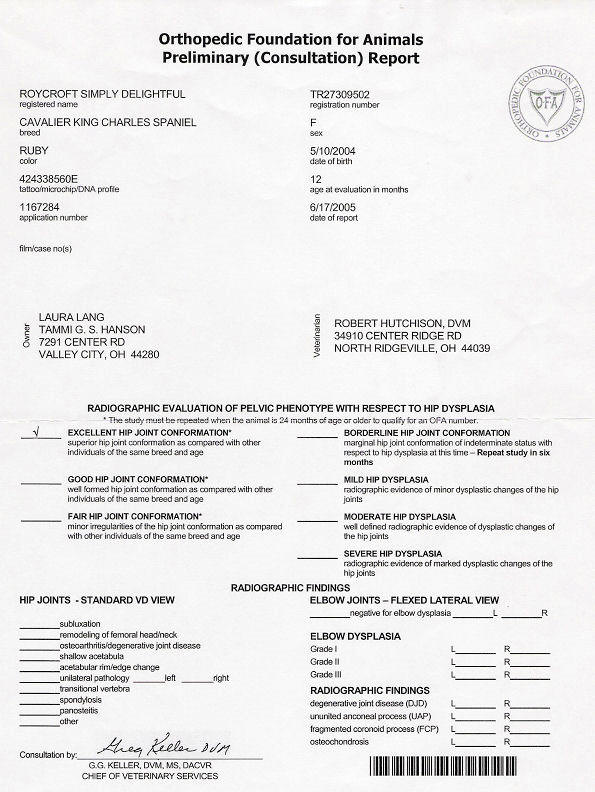
OFA uses the following method of classifying hip dysplasia. A
clear x-ray of the hips is taken and sent to OFA for evaluation.
Preliminary x-rays (taken before the dog is age 2) are evaluated
by one radiologist. Permanent x-rays (taken after the dog is 2
years old) are evaluated by three radiologists who have to come
to an agreement on the status of the hips. Hips declared free of
hip dysplasia are assigned either an Excellent, Good or Fair
rating. There is a Borderline Conformation/Intermediate
classification in which they normally ask that the dog be
x-rayed again at a later date for re-evaluation. Hips that are
dysplastic are rated as Mild, Moderate or Severe. OFA suggests
that only dogs FREE of any signs of hip dysplasia in the x-rays
should be used for breeding.
Below are hip x-rays of Cavaliers showing most of the grades of
classification. I don’t have a copy of a Borderline or a Severe.
You can find examples from other breeds online if you are
interested. You can easily see in each x-ray how there is less
and less coverage of the head of the femur (the femoral head—the
round ‘ball’ at the ‘top’ of the leg bone) and the acetabulum
(the ‘cup’ where the femoral head sits) gets more shallow as the
status of the hips declines until they barely overlap at all. In
a severe there is basically no overlapping whatsoever.
PennHIP uses an entirely different way of evaluating hips. They
have the vet take 3 different x-rays in 3 different positions to
check for laxity of the hip joints. A number is assigned to each
hip stating the amount of laxity found. PennHIP then publishes
the *average* hip scores for that particular breed. They suggest
that only dogs that have laxity scores in the *better* half
should be used for breeding. Obviously, although the aim is at
improving the hip status of offspring, some dysplastic dogs may
be able to be used for breeding under the PennHIP approach,
especially in breeds prone to a lot of hip dysplasia. This is a
more controversial approach, but their hope is that laxity is
the prime reason for the development of hip dysplasia and using
dogs with the lower laxity scores may possibly bring about
improvement in the breed more quickly.
Treatment for hip dysplasia is directed at relieving pain and
improving function by giving aspirin or one of the newer
products used in the treatment of degenerative joint disease. If
pain cannot be controlled, there are surgical procedures which
may relieve pain and improve function in some individuals.
For more information on hip dysplasia, please see some of the
following websites:
www.ofa.org/
www.vet.upenn.edu/pennhip/
The following are the only acceptable result forms for hip
dysplasia in the USA:
Below is the OFA Hip Clearance Form
NOTE O.F.A. NUMBER ON FORM
As an interesting comparison, the following is a picture of the
x-ray of the same dog, this time submitted to OFA for
evaluation. OFA evaluated her hips as *Fair*.
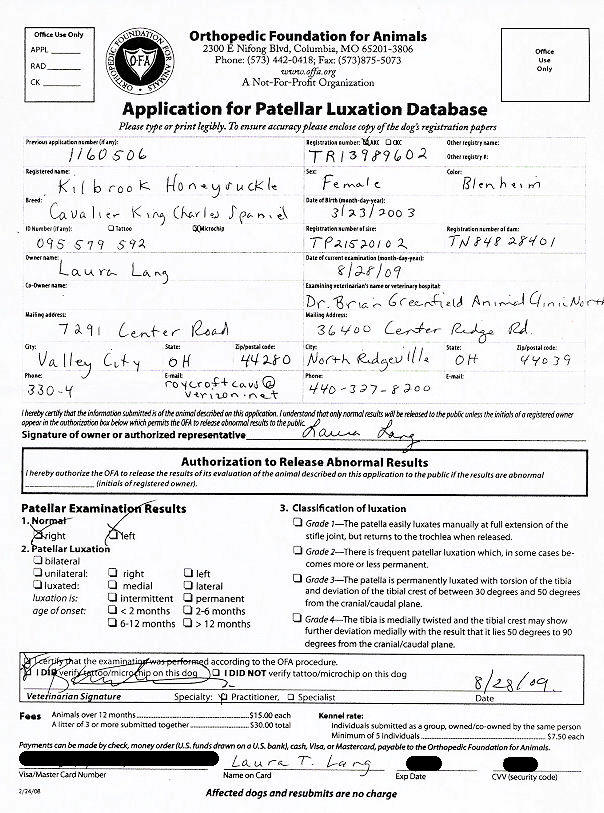
PATELLAR LUXATION or dislocating
kneecap(s) can be inherited, or acquired through trauma.
It occurs sporadically among Toy breed dogs, although it can be
found in large breeds.
In dogs the patella is a small bone which protects the front of
the stifle joint; it is the counterpart of the kneecap in humans.
It is anchored in place by ligaments, and slides in a groove in
the femur.
Conditions which predispose to patellar luxation are: a
shallow groove, weak ligaments; and mal-alignment of the tendons
and muscles that straighten the joint. The patella may
slip inward (medial luxation) or outward (lateral luxation).
Luxating patellas in toy breeds are most commonly found to
luxate medially. Lateral luxation is most commonly caused
by trauma, although in some cases it can also be inherited.
The signs of patellar luxation are difficulty straightening the
knee; pain in the stifle; and a limp. Often a dog with
patellar luxation will look somewhat stiff in that leg because
the dog is attempting to use muscles to *lock* it so the patella
won't move around as much.
The diagnosis is confirmed by a regular veterinarian who
manipulates the stifle joint and is able to push the kneecap in
and out of position without excess force.
There are 4 grades of patellar luxation:
(1) Intermittent patellar luxation causing the limb to be
carried occasionally.
(2) Frequent patellar luxation which, in some cases, becomes
more or less permanent.
(3) The patella is permanently luxated with torsion of the tibia
and deviation of the tibial crest of between 30 degrees and 50
degrees from the cranial/caudal plane.
(4) The tibia is medially twisted and the tibial crest may show
further deviation medially with the result that it lies 50
degrees to 90 degrees from the cranial/caudal plane.
Grades (1) and (2) can often be controlled by keeping the dog
lean, on a good diet (supplements may help as well), and not
allowing excessive jumping. A Grade 2 can tighten to a
Grade 1 and often a Grade 1 can tighten until there is no
patellar luxation at all. They can also get worse.
Grades (3) and (4) nearly always need surgery to deepen the
groove and/or realign or tighten the ligaments.
Any licensed veterinarian can manipulate and check for patellar
luxation. X-rays are not necessary.
NOTE THE O.F.A. NUMBER ON FORM |








Copyright 2023 Roycroft Cavaliers
No part of this site may be copied or reproduced without written permission.